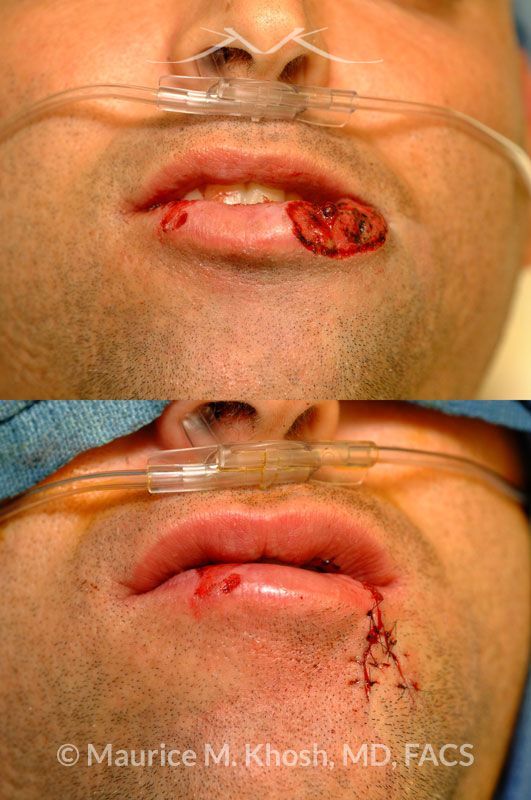
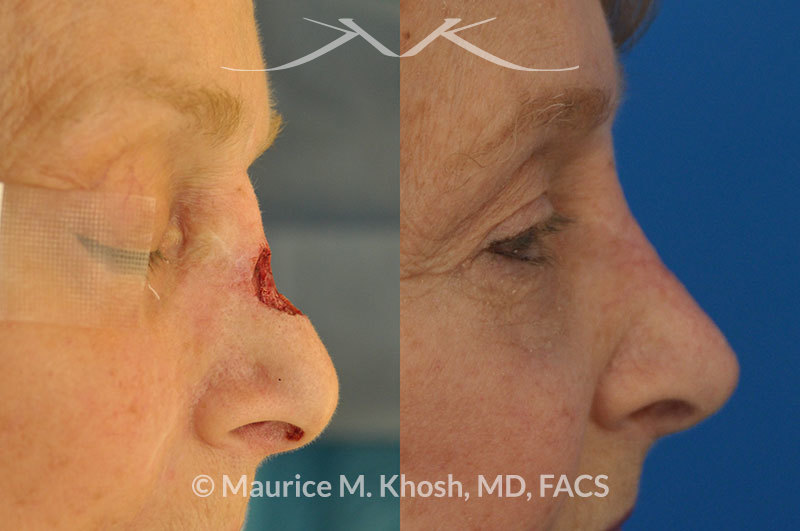
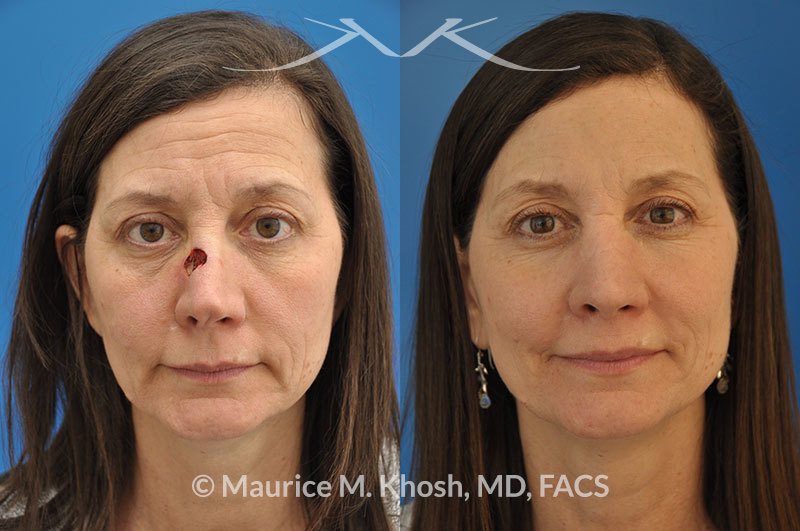
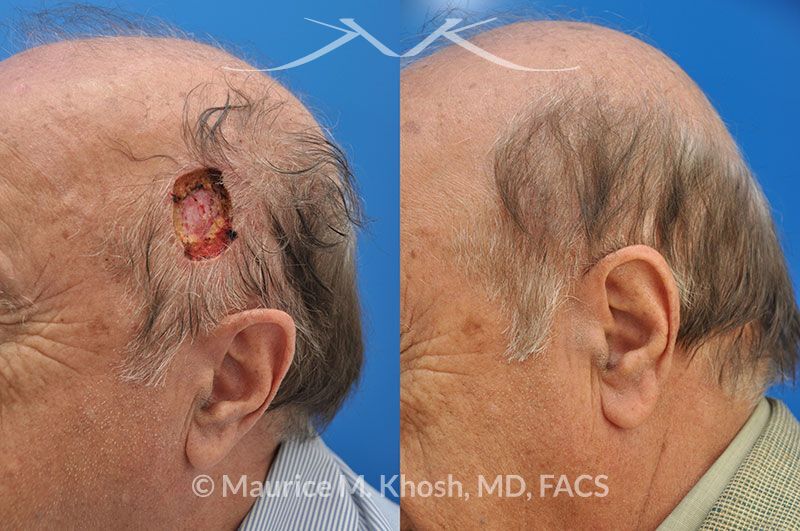
Moh’s Skin Cancer Reconstruction
Before and After Gallery







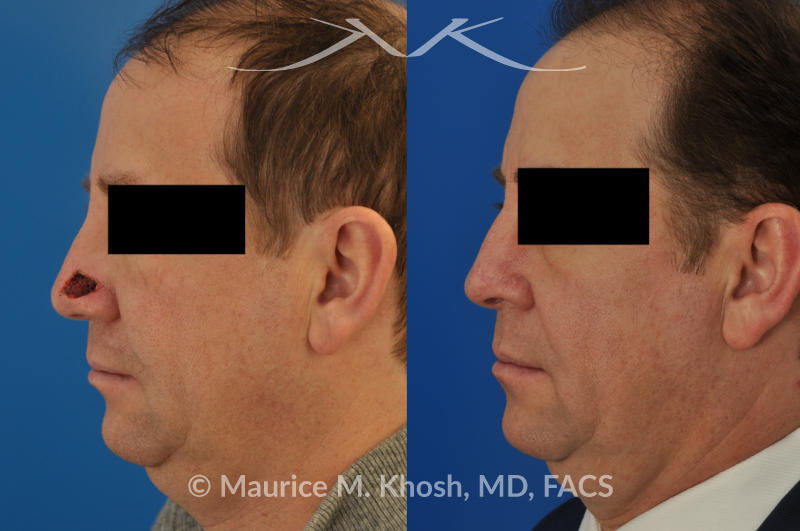

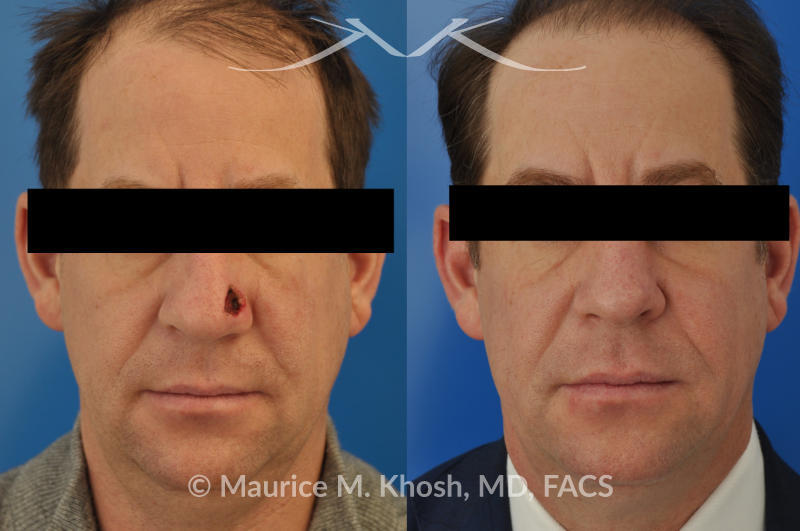

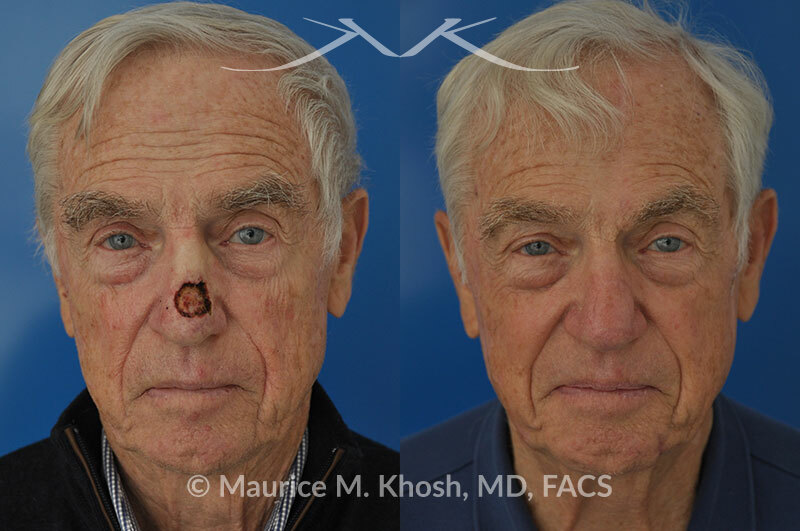


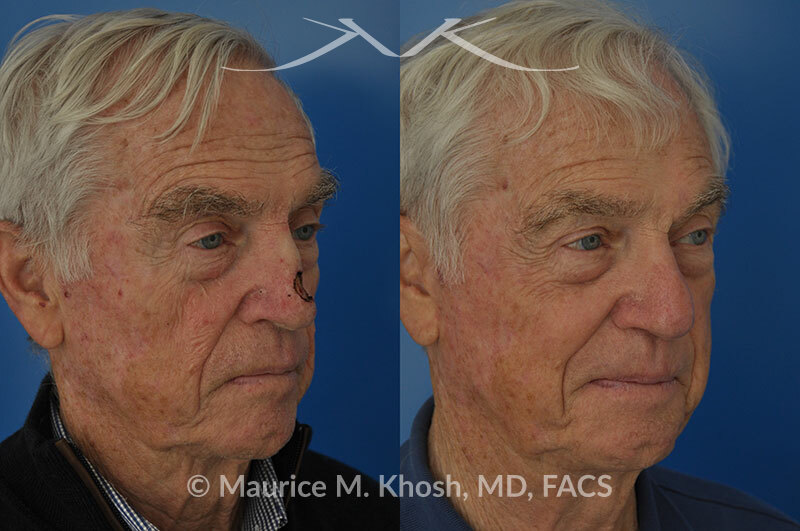
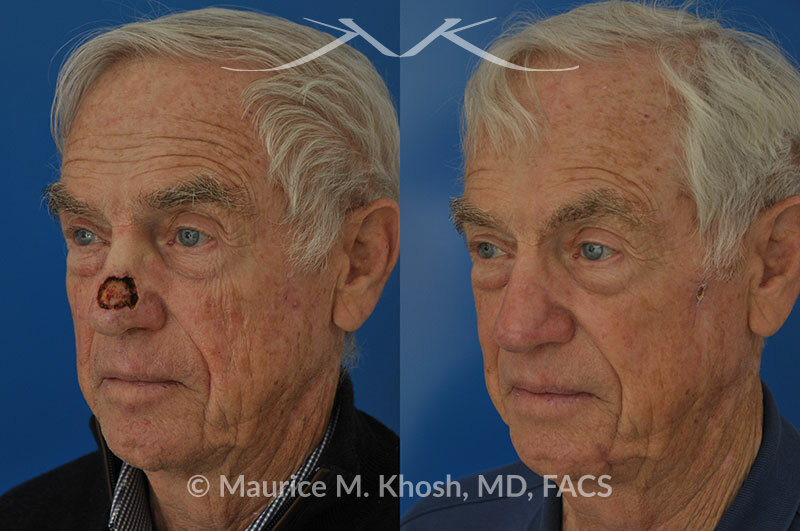










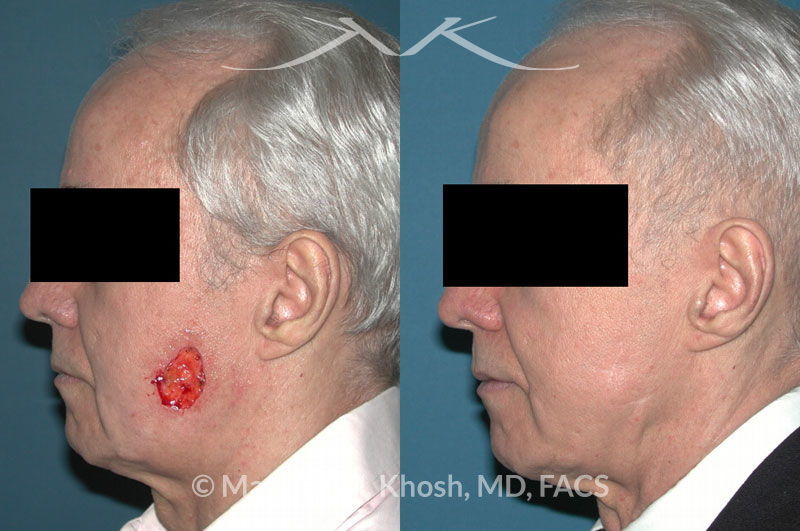
































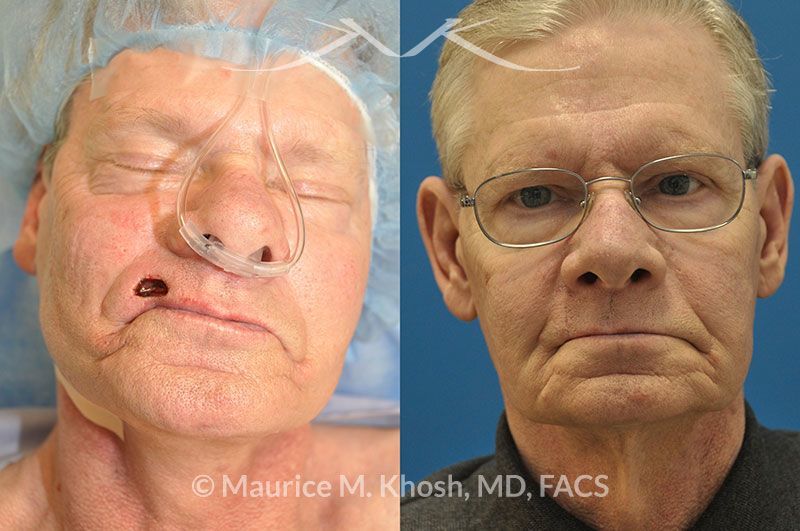













































































Disclaimer: These are actual results for patients of Dr. Maurice Khosh. Plastic and cosmetic surgery results can vary between patients.
Disclaimer: These are actual results for patients of Dr. Maurice Khosh. Plastic and cosmetic surgery results can vary between patients.
Based on 174 reviews
Meredith G.Saw Dr. Khosh for a fractured nose. He reset my nose beautifully (and with little discomfort to me) and then discussed some of my sinus issues with me upon my follow up visit. Never felt like he was rushing me out and felt very confident in his abilities. I would highly recommend to anyone needing plastic or reconstructive options!
Jackie C.Great front office, really good experience after what was a terrible accident. I was made to feel comfortable. Dr. Khosh is very good at what he does. I'm still healing but I'm confident of the results
Kaitlin M.Dr. Khosh takes exceptional care of his patients. He has operated on me twice, each time making me feel extremely comfortable and satisfied with the results. His staff is also very kind and knowledgeable.
Diana G.Dr. Khosh & his staff Susan & Christine are absolutely amazing! They were so supportive & helpful from beginning to end & they are just wonderful people. Thank you guys I truly appreciate everything you guys have done for me. I would recommend them to anyone & everyone!
Joann M.After visiting and being evaluated by several doctors, I kept going back to Dr. Khosh. His tranquil spirit and professionalism were captivating. Thank you for a job well done and keeping me calm throughout the entire process. A special thanks to your staff Susan and Christine for all of their support as well. Hi highly recommend Dr. Khosh.
Leah G.Upon hearing of the overwhelmingly positive experience a friend of mine had in choosing Dr. Khosh as her surgeon, I decided to make an appointment for my own septoplasty/rhinoplasty/turbinate reduction. Although I was slightly skeptical as the praise I had heard seemed a bit hyperbolic, all uncertainty dissipated after meeting the Doctor and his staff. My pre- and post-operative experience was excellent in terms of concerns adequately addressed prior to the surgery and mitigation of any bruising in the convalescent period. Despite my apparent predisposition to rather slower healing, a year after the surgery, my nose looks really pretty and my breathing entirely unobstructed! I highly recommend Dr. Khosh!
Courtney G.AMAZING!!!!!! I had Dr Khosh perform lipo on my chin/neck and my result is unbelievable! Better than I could have expected! I met with a couple of surgeons and the second I met with Dr Khosh I knew he was the one I was going with. He was compassionate and explained every detail of what would take place during the surgery and what to expect during recovery. I even emailed a few times during recovery with various questions and he got right back to me asap which was really comforting! I honestly fully recommend Dr Khosh, he did an amazing job and is an amazing person.
Frieda S.i can finally breathe!! Dr. Khosh made the entire experience a breeze, it was truly a pleasure to be under his care. I am forever thankful and highly recommend him. Not only does his work speak for himself, but he has excellent bedside manner. His kindness and patience is above and beyond. He takes the time to answer to every question you have to help you understand the process while at the same time making you feel so comfortable. From the first consultation i knew i was in good hands. I am so pleased with the result and forever thankful.